















SMS – Solutions Made Simple
الحلول المبسطة لسلامة المريض
|
 |
| PPS – Patients for Patient Safety
بطاقة سمعنا صوتك
|
 |
| Patient Safety Stories Resource booklet of 36 true patient safety incidents. 2014
أحداث حقيقية لسلامة المرضى
|
 |
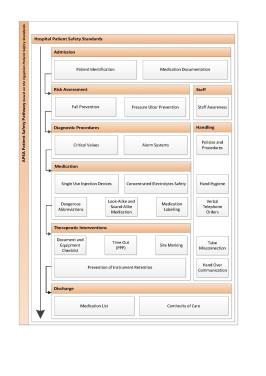
| Patient Safety Pathway Patient safety practices for hospital and primary care patients. 2014
المسار الآمن للمريض
|
 |
| Patient Safety Friendly Hospital
APSA Starter Version
2013 |
 |
| Patient Safety Friendly Hospital
WHO Initiative
2011 - 2012 |
 |
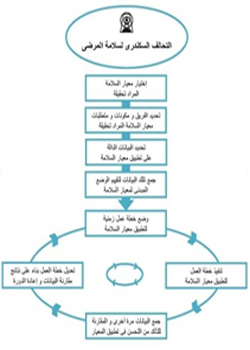
| Operating Room Audit Project (ORAP) May 2012 مشروع تقييم الممارسة الآمنة بحجرات العمليات
|
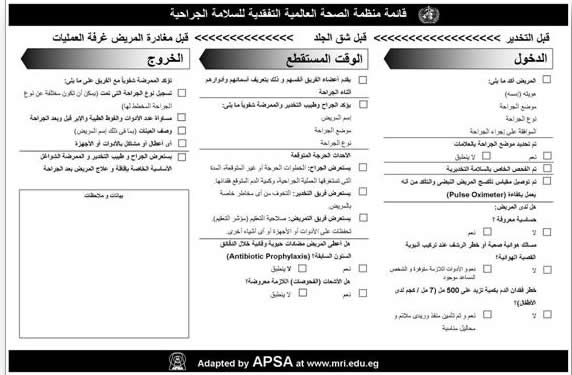 |
| Surgical Safety in the Operating Room December 2014, Gamal Abd El Nasser Hospital, Health Insurance Organization, Alexandria May 2012 ورشة عمل عن السلامة الجراح ية داخل حجرات العمليات
|
 |
| Pressure Ulcer Prevention Symposium October 2013, Gamal Abd El Nasser Hospital, Health Insurance Organization, Alexandria
ورشة عمل عن الوقاية من قرح الفراش
|
 |
| Fall Prevention Symposium November 2012, Gamal Abd El Nasser Hospital, Health Insurance Organization, Alexandria
|
 |
| Event Management and Analysis february 2012, Medical Technology Centre, Medical Research Institute, University of Alexandria
ورشة عمل عن إدارة و تحليل الأحداث
|
 |
| Event Management and Analysis January 2012, Medical Technology Centre, Medical Research Institute, University of Alexandria ورشة عمل عن إدارة و تحليل الأحداث
|
 |
| Clinical Risk Management Workshop April 2011, Medical Research Institute, University of Alexandria.
ورشة عمل عن تقييم المخاطر الإكلينيكية
|
 |
| Clinical Risk Management Workshop February 27-28, 2011, Medical Research Institute, University of Alexandria.
ورشة عمل عن تقييم المخاطر الإكلينيكية
|
 |
| Hand Hygiene Forum March 11, 2010, Medical Research Institute, University of Alexandria. منتدى نقاش عن نظافة الأيدى
|
 |
| Adverse Event Measurement Workshop (WHO - APSA) November 2-5, 2009. Suzanne Mubarak Centre, Alexandria and Medical Research Institute, University of Alexandria.
ورشة عمل عن قياس الأحداث السلبية
|
 |
| Audit Medical Records October 17-18 , 2009. Abou Keir Hospital. Ministry of Health. Alexandria. مراجعة ملفات المرضى – مستشفى أبى قير
|
 |
| Audit Medical Records October 14-15, 2009. Gamal Abdel Nasser Hospital. Medical Insurance Organisation. Alexandria. مراجعة ملفات المرضى – مستشفى جمال عبد الناصر
|
 |
| Audit Medical Records October 10-11, 2009. Shark El-Madinah Hospital. Medical Ministry of Health. Alexandria. مراجعة ملفات المرضى – مستشفى شرق المدينة
|
 |
| Medical Records Units Audit Workshop August 19-20, 2009. Faculty of Medicine, Alexandria. ورشة عمل عن كيفية تقييم أقسام السجلات الطبية
|
 |
| Medical Records Units Audit Workshop July 14-15, 2009 Medical Insurance Organization, Alexandria. ورشة عمل عن كيفية تقييم أقسام السجلات الطبية
|
 |
| Surgical Safety Awareness Meeting April 27, 2009. Medical Research Institute. لقاء مفتوح عن السلامة الجراحية
|
 |
| Patient Safety awareness meeting May 7, 2009. Medical Research Institute. لقاء مفتوح عن سلامة المريض
|
 |
Institute News
News Archive
- Woman inner peace and family general health seminar announcement
- The 2nd Conference of Medical Biophysics and its Applications
- Handwashing awareness
- 6th october artistic and cultural competition announcement
- leukemia Awareness Month Sceitific day
- Students Orientation Autumn 2025/26
- 6th October celebration
Students News
Students News Archive
- MRI Postgraduate application extension till 21 Aug...
- GraphPad Prism as a statistical tool for biomedica...
- Tools of References Management " EndNote "
- MRI Postgraduate application procedures
- Exam Schedule Spring 2025
- The Fourth Student Conference of the Medical Resea...
- Announcement for new students, registration spring...
Conferences
Archive
APSA activity
---- ----- ---- ----- ---- ----
high alert drugs
| High-Alert Medications | الأدوية الخطرة |
| As listed by the Institute for Safe Medication Practices | |
| Classes / Categories of Medications | تصنيفات الادوية |
| Adrenergic agonists, IVeg, epinephrine, phenylephrine, norepinephrine | المنبهات الأدرينية الوريدية |
| Adrenergic antagonists, IVeg, propranolol, metaprolol, labetalol | المقاومات الأدرينية الوريدية |
| Anesthetic agents, general, inhaled, IVeg, propofol, ketamine | الأدوية التخديرية (البنج الكلى) المستنشقة و الوريدية |
| Antiarrhythmics, IVeg, lidocaine, amiodarone | موانع إضطراب ضربات القلب الوريدية |
| Antithrombotic agents (anticoagulants)Including warfarin | موانع التجلط |
| Cardioplegic solutions | محاليل شل القلب |
| Chemotherapeutic agents, parentral, oral | الأدوية الكيميائية الوريدية و الفمية |
| Dextrose, hypertonic, 20% or greater | دكستروز 20% أو أكثر |
| Dialysis solutions, peritoneal, hemodialysis | محاليل الغسيل الكلوى البريتونى و الدموى |
| Epidural or intrathecal medications | حقن الأدوية داخل الفوق الجافية أو داخل القراب |
| Hypoglycaemics, oral | مخفضات سكر الدم الفمية |
| Inotropic medications, IVeg, digoxin, milrinone | الأدوية المؤثرة على عضلة القلب الوريدية |
| Liposomal forms of drugseg, liposomal amphotericin B | الأدوية الشحمية الشكل |
| Moderate sedation agents, IVeg, midazolam | المهدئات الوريدية |
| Moderate sedation agents, oral, childrene.g. chloral hydrate | المهدئات الفمية للأطفال |
| Narcotics / opiates, IV, dermal, oralliquid, immediate, sustained-release forms | المخدرات و الأفيونات الوريدية و الجلدية و الفمية |
| Neuromuscular blocking agentseg, succinylcholine, rocuronium, vecuronium | الأدوية المانعة للتوصيل العصبي العضلي |
| Radiocontrast agents, IV | أدوية تباين الأشعة الوريدية |
| Total parentral nutrition solutions | محاليل التغذية الوريدية الشاملة |
| High-Alert Medications | الأدوية الخطرة |
| As listed by the Institute for Safe Medication Practices | |
| SpecificMedications | أدوية بذاتها |
| Colchicine injec | حقن الكولشيسين |
| Epoprostenol , IV | الإيبوبروستينول الوريدى |
| Insulin , Subctaneous and IV | الإنسولين التحت الجلدى والريدى |
| Magnesium sulphate injection | حقن كبريتات الماغنسيوم |
| Methotrexate , oral , non – oncologic use | الميثوتركسات الفمى و للإستخدام فى غير الأورام |
| Opium tincture | صبغة الأفيون |
| Oxytocin , IV | الأوكسيتوسين الوريدى |
| Nitroprusside sodium for injection | صوديوم النيتروبرسيد للحقن |
| Potassium chloride , injection concentrate | حقن كلوريد البوتاسيوم |
| Potassium phosphate injection | حقن فوسفات البوتاسيوم |
| Promethazine , IV | البروميثازين الوريدى |
| Sodium chloride for injection | كلوريد الصوديوم للحقن |
| Hypertonic saline (>0.9 % concentration ) | محاليل الملح عالية التركيز |
| Water for injection, inhalation , irrigation 100 ml containers or more | ماء للحقن أو الإستنشاق أو الغسيل فى عبوات 100 ملى أو أكثر |
Download
![]()